
CHEMICAL COORDINATION AND INTEGRATION
INTRODUCTION
- Endocrine system comprises of endocrine glands and their hormones.
- Though different endocrine glands are different in embryonic origin and are isolated from one another but these interact with one another to collectively form an endocrine system.
- Animals have three types of glands – exocrine, endocrine and heterocrine.
- Exocrine glands have ducts for discharging their secretions. Therefore, they are called as duct glands. E.g., liver, sweat gland, sebaceous gland, gastric glands and some intestinal glands.
- Endocrine glands lack ducts and pass secretions into the surrounding blood directly. Therefore, they are called ductless glands. E.g., thyroid, parathyroid, adrenal, pituitary, pineal body and thymus.
- Heterocrine glands consist of both exocrine and endocrine tissue. The exocrine discharge its secretion by a duct and the endocrine tissue discharges its secretion into the blood. Pancreas and gonads are heterocrine glands. These are also called mixed glands.
- Endocrinology is the study of endocrine glands, hormones & endocrine system.
- Father of endocrinology was Thomas Addison.
- Endocrine system in association with nervous system functions in a coordinated way to maintain homeostatic state within the body.
Table : Difference between Nervous and Endocrine Co-ordination

HORMONES
- Hormone is a chemical produced by endocrine glands and released into the blood and transported to a distantly located target organ.
- Hormones are non-nutrient chemicals which act as intercellular messengers and are produced in trace amounts.
- First hormone discovered was secretin. It was discovered by two English physiologists : William M. Bayliss and Ernest H. Starling in 1903.
- A hormone which stimulates another endocrine gland to secrete its hormone is called trophic hormone.
- Term hormone was coined by Starling (1905) from Greek word hormone means to excite. It is a misnomer because a number of hormones are known to have inhibitory effect (e.g., somatostatin).
PROPERTIES OF HORMONES
- These are secreted by endocrine gland (biogenic in origin).
- Their secretions is released directly into blood (except local hormones, e.g., gastrin).
- These are carried to distantly located specific organs, called target organ.
- These have specific physiological action (excitatory or inhibitory). These co-ordinate different physical, mental and metabolic activities and maintain homeostasis.
- The hormones have low molecular weight, e.g., ADH has a molecular weight of 600-2000 daltons.
- These act in very low concentration.
- Hormones are non-antigenic means that they cannot stimulate the production of antibodies.
- These are mostly short-lived, so have no cumulative effect.
- Some hormones are quick acting, e.g., adrenaline, while some act slowly, e.g., oestrogen of ovary.
- Some hormones are secreted in an inactive form called prohormone, e.g., pro-insulin.
- Hormones after their action are destroyed in liver and kidney.
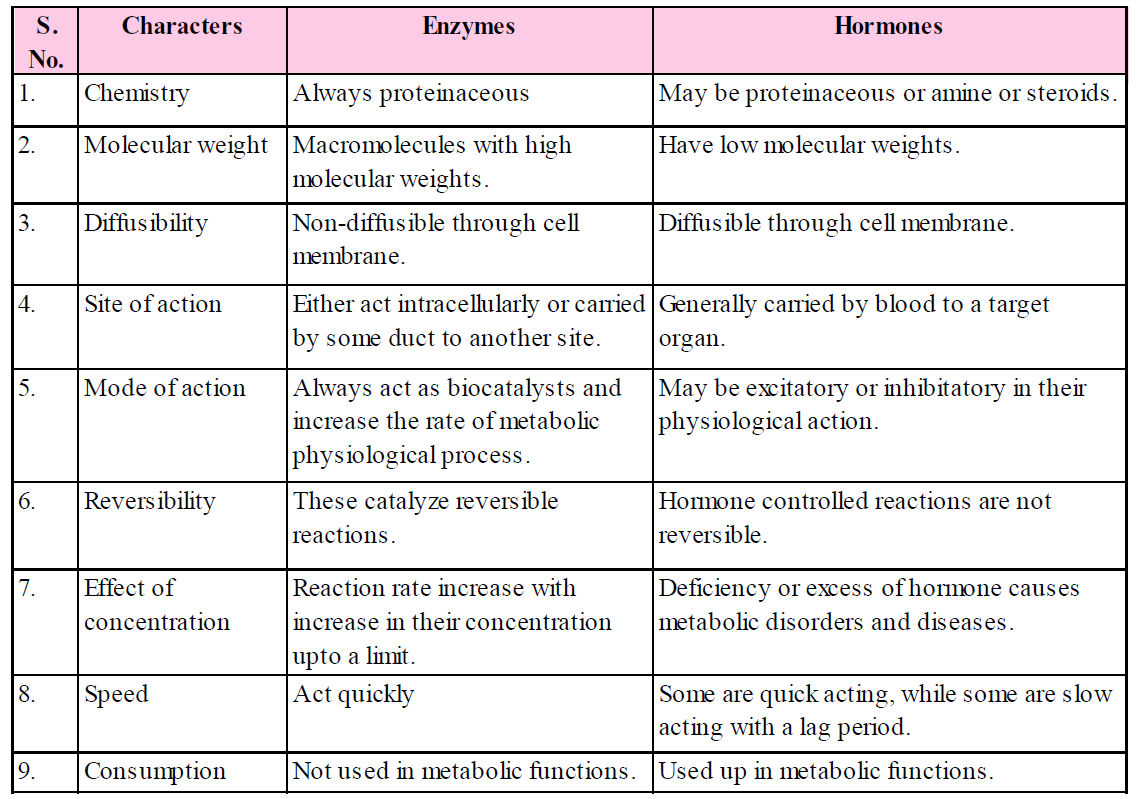
HORMONES VS ENZYMES
Similarities between hormones and enzymes are :
- Easily soluble and diffusible.
- Not obtained from the food, but synthesized by the body.
- Required and secreted in minute quality.
- Not stored (except thyroxine) and have high specificity.
Table : Difference between hormone and enzymes
HUMAN ENDOCRINE SYSTEM
- Endocrine system of human consists of various endocrine glands present in different regions of the body.
- The major glands that form human endocrine system are the hypothalamus, pituitary gland, pineal, thyroid, parathyroid, thymus, adrenal gland, pancreas, testes and ovaries.
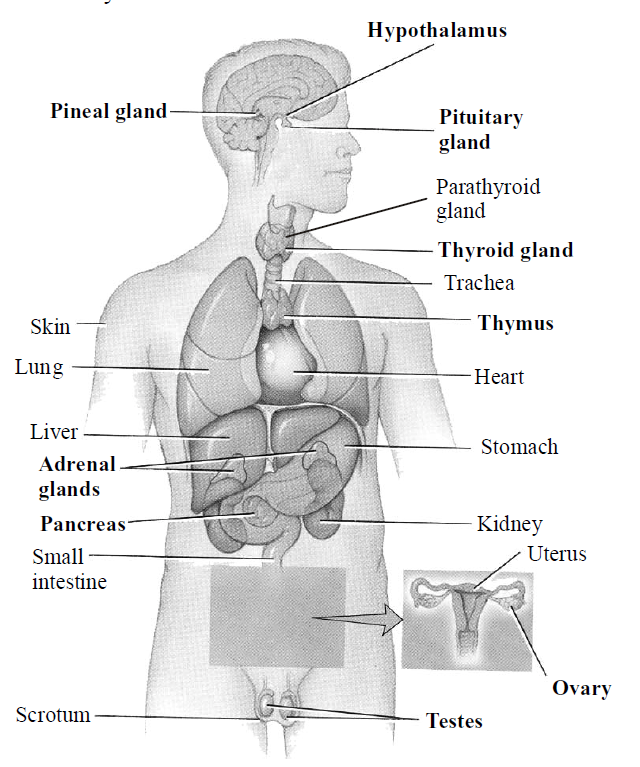
Fig. : Endocrine glands
HYPOTHALAMUS
- The hypothalamus is a part of the forebrain and appeared as the floor of the diencephalon. It is the main link between the endocrine and nervous system.
- It contains several groups of neurosecretory cells (called hypothalamic nuclei) which produce hormones (called neuro-hormone). These hormones regulate the synthesis and secretion of pituitary hormones.
The hormones produced by the hypothalamus are of two types – the releasing hormones which stimulate secretion of pituitary hormones (called trophic hormones) and the inhibiting hormones which inhibit secretions of pituitary hormones.
- Hormones originating in the hypothalamic neurons, pass through axons and are released from their nerve endings. Hormones reach the pituitary gland through a portal circulatory system and regulate the functions of the anterior pituitary. The posterior pituitary is under the direct neural regulation of the hypothalamus.
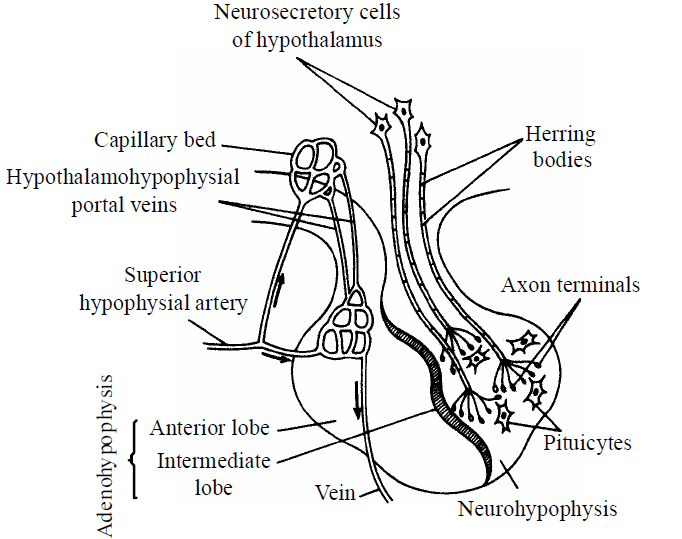
Fig. : Blood supply to pituitary
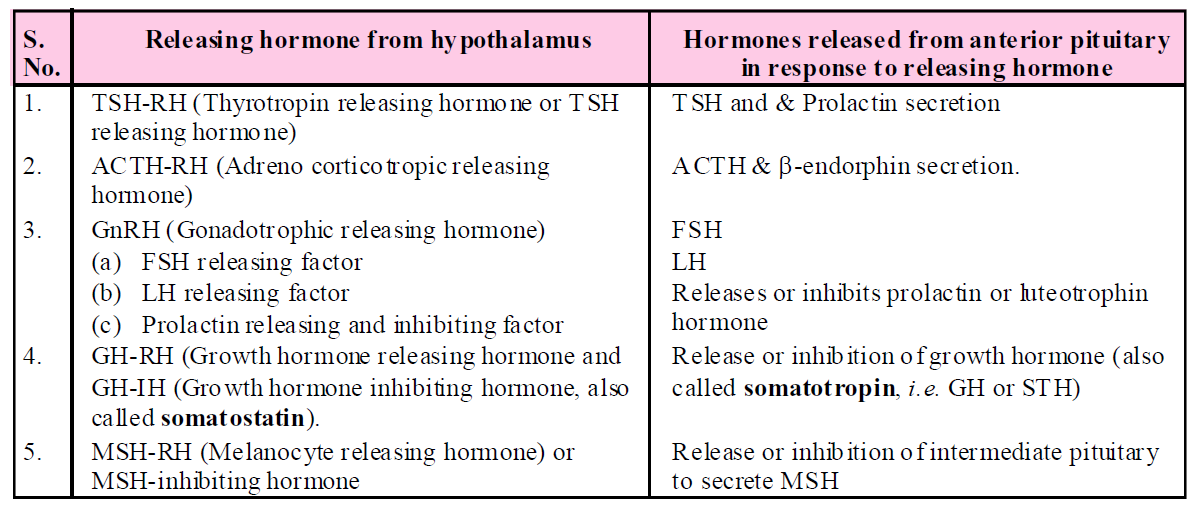
Table : Specific hormone released by the hypothalamus and their effect on pituitary gland
PITUITARY GLAND
- The pituitary gland, located in a bony cavity called sella turcica and is attached to the floor of Diencephalon (forebrain) through a stalk.
- The pituitary gland plays most important regulatory role in the body. Besides regulating growth, sex and general behaviour, it also regulates the secretory activities of other principal endocrine glands and cells. Most appropriately, therefore, pituitary has been referred to as "The Master gland" of body, or the "Chief Executive of Endocrine System", or "The Leader of Endocrine Orchestra".

Fig.: Diagram to show the hormones of the pituitary gland and their target tissues and organs
- Pituitary gland is divided into two parts–adenohypophysis and neurohypophysis.
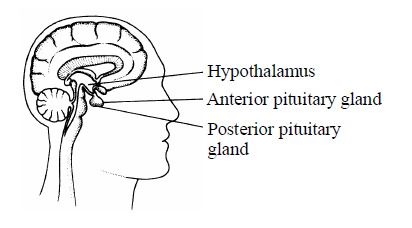
Fig. : Location of pituitary gland
- Adenohypophysis is formed of 3 parts – pars distalis, pars tuberalis and pars intermedia.
- The pars distalis and pars tuberalis region of pituitary are commonly called anterior pituitary.
- Hormones of the anterior pituitary are growth hormone (GH), thyroid stimulating hormone (TSH), follicle stimulating hormone (FSH), luteinizing hormone (LH), interstitial cell stimulating hormone (ICSH), prolactin (PRL) and adrenocorticotropic hormone (ACTH).
- Growth hormone stimulates the liver to form "somatomedins" ("Insulin like growth factors"). These somatomedins have potent effect on bone growth.
- Pars intermedia secretes melanocyte stimulating hormone (MSH).
- In humans, the pars intermedia is almost merged with pars distalis.
- Neurohypophysis has three main parts – pars nervosa (infundibular process), median eminence and infundibular stalk.
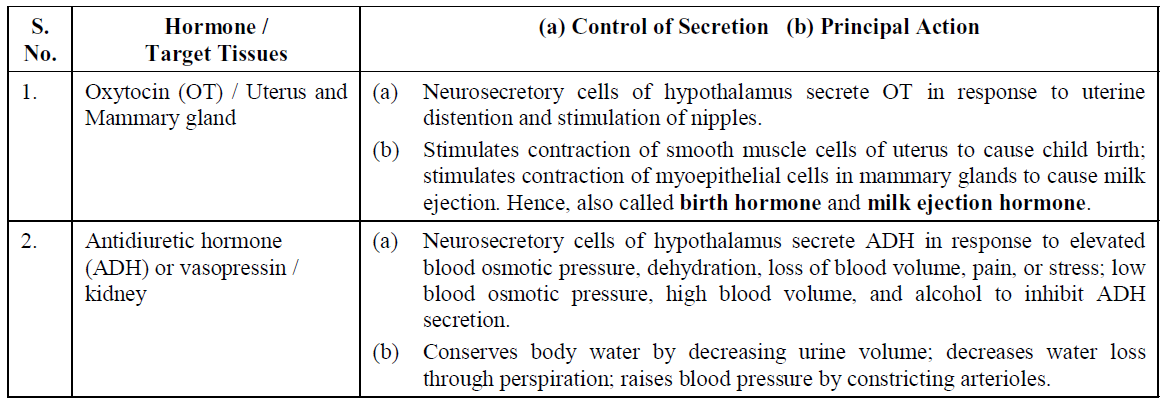
- Neurohypophysis (pars nervosa) is also known as posterior pituitary. It stores and releases two hormones - oxytocin and vasopressin, which are actually synthesized by the hypothalamus and are transported axonally to neurohypophysis.
Table : Anterior Pituitary Hormones
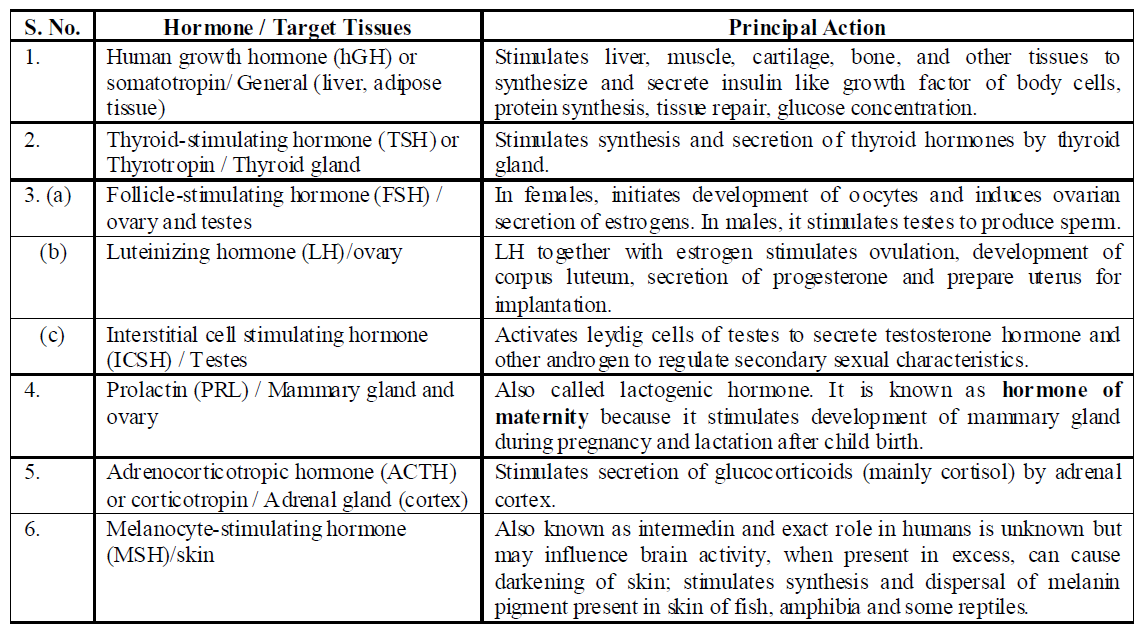
Table : Posterior Pituitary Hormones
DISORDERS OF GROWTH HORMONE
- Hypersecretion of GH stimulates abnormal growth of the body leading to gigantism and acromegaly whereas hyposecretion of GH results in stunted growth resulting in pituitary dwarfism and simmond’s disease.
- Proportionate gigantism : Hypersecretion (oversecretion of growth hormone) during growth period (childhood and adolescence) causes excessive growth (hypergrowth) of all body parts, resulting into a symmetrically giant body. This is called proportionate gigantism.
- Acromegaly : It occurs in adults. In this, the long bones do not grow in length due to closed epiphyseal plate at their ends, but the bones of hands, feet, lower jaw and rib cage thicken. Simultaneously, eyelids, lips, tongue, nose, chin, etc. also enlarge. Soles, palms and forehead become wrinkled. Skin thickens, becomes wrinkled, coarse and fluffy (hirsutism). Consequently, the body becomes ugly like a gorilla. This is called disproportionate gigantism or acromegaly. It is common in men and rare in women.
- Nanism or ateliosis : Hyposecretion (undersecretion) of growth hormone in childhood results into a blunted growth of body. Growth of all organs is retarded. Growth of bones at their epiphysial end stops. Hence, the bones do not grow in length, so that the body remains a dwarf. This pituitary dwarfism is called nanism or ateliosis. The dwarf are called midgets.
- Simmond’s disease is a rare condition in adults in which patients become thin and show signs of premature ageing.
DISORDER OF THYROID STIMULATING HORMONE
Hyposecretion of TSH leads to thyroid atrophy while hyperactivity produces symptoms similar to Grave’s disease.
DISORDER OF ACTH
Hypersecretion of ACTH leads to rheumatoid arthritis while hyposecretion leads to excessive growth of adrenal cortex.
DISORDERS OF GONADOTROPINS
Hyposecretion of ICSH results in impaired development of external genitalia and LH results in sterility in females and FSH results in failure of gamete formation.
DISORDERS OF PROLACTIN
Hypersecretion of prolactin
- May hinder menstruation
- May cause impotency.
- In pigeons and doves, it stimulates the epithelial cells of crop in both males and females to secrete "pigeon milk" for nutrition of newly hatched infants.
DISORDER OF ANTIDIURETIC HORMONE (ADH)
- Hyper secretion of ADH causes diabetes insipidus. It is characterised by micturating dilute urine several times a day which results in excessive thirst (polydipsia) and dehydration.
- Alcohol inhibits secretion of ADH, so increases urine output, increase in the count of erythrocyte, amount of haemoglobin etc.
PINEAL GLAND
- Pineal gland is composed of modified nerve cells called pinealocytes.
- It is a stalked small rounded gland and can be found deep in the brain at the top of the third ventricle (called pineal recess) where it has close communication with the cerebrospinal fluid. Due to its position, it is also called epiphysis cerebri.
- Pineal secretes two biogenic hormone - melatonin and serotonin.
- Melatonin plays a very important role in integrating photoperiod and affecting circadian rhythms. For example, it helps in maintaining the normal rhythm of sleep-wake cycle, body temperature. In addition, melatonin also influences metabolism, pigmentation, the menstrual cycle as well as our defense capability.
- Light falling on the retina of the eye decreases melatonin production, darkness stimulates melatonin synthesis. Girls blind from birth attain puberty earlier than normal, apparently because there is no inhibitory effect of melatonin on ovarian function.
- Melatonin is also a potent antioxidant. Melatonin causes atrophy of gonads in several animals.
- Serotonin acts as vasoconstrictor and helps to decrease the diameter of blood vessel.
THYROID GLAND
- The thyroid gland are located on either side of the trachea.
- It is bilobed and both the lobes are interconnected with a thin flap of connective tissue called isthmus.
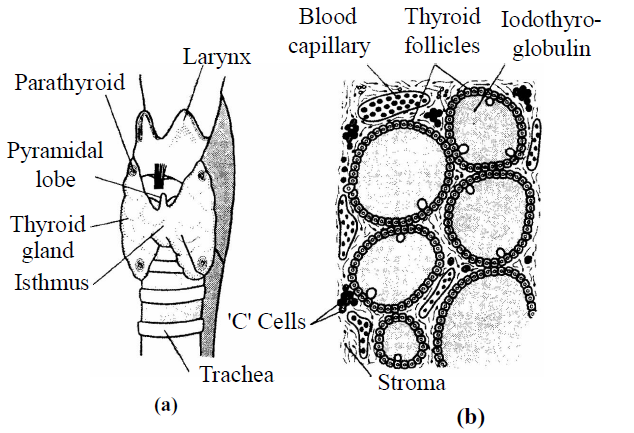
Fig. : (a) Thyroid gland, (b) Follicles suspended in stroma of a lobule
- Thyroid gland is the largest endocrine gland in the body.
- Endostyle of lower vertebrates like Herdmania, Amphioxus is homologous of thyroid gland.
- Thyroid is the only endocrine gland in the body which stores its hormone in its inactive state.
- Thyroid follicles contain thyroglobulin. Thyroglobulin is a large protein molecule that contain multiple copies of one amino acids tyrosine.
- These follicular cells secretes two hormones - tetraiodothyronine or thyroxine (T4) and triiodothyronine (T3).
- The thyroid needs iodine to produce these hormones.
- For secreting the iodinated hormones in normal amounts, the thyroid daily utilizes about 150 micrograms (0.15 milligram) of iodine. Obviously, a person must daily obtain 150mg of iodine from food. We can obtain this from dairy products, drinking water, seafood, etc. If obtained more than this, we excrete the excess iodine in urine.
- Iodine in food is absorbed and circulated in blood in the form of iodide ions (I–). Follicular cells of thyroid very actively obtain these ions from blood by active transport. That is why, the concentration of I– in these cells normally remains about 50 to 250 times more than in blood. These cells possess peroxidase enzyme in abundance. Peroxidase continuously oxidizes iodide ions into molecular iodine (2I– → I2). Iodine is, then, released by follicular cells into follicular cavity.
- Thyroid hormones plays an important role in regulating basal metabolic rate and calcium balance. These hormones also support the process of red blood cell formation and control the metabolism of carbohydrates, proteins and fats. Maintenance of water and electrolyte balance is also influenced by thyroid hormones.
- Thyroxine stimulates the metamorphosis of tadpole larva in amphibians.
- Thyroid tissue is made up of two types of cells– follicular cells and parafollicular cells.
- Parafollicular cells are groups of endocrine cells scattered in the connective tissue and between the thyroid follicles.
- Parafollicular cells of the thyroid gland also secretes a non-iodinated protein hormone called thyrocalcitonin (TCT) which regulates the blood calcium levels.
- Calcitonin (thyrocalcitonin) plays an important role in calcium and phosphorus metabolism. In particular, calcitonin has the ability to decrease blood calcium levels at least in part by effects on two well studied target organs-bone & kidney.
- The BMR of normal adult man is 40 cal/m2 and 37.5 cal/m2 in woman.
DISORDERS OF THYROID GLAND
Hyposecretion of thyroid hormones lead to cretinism, myxoedema, simple goitre and hashimoto’s disease, whereas hypersecretion leads to Grave’s disease (exophthalmic goitre).
- Cretinism : It is a disease of infants, called cretins. It is characterised by decreased BMR (50% than normal); stunted growth; retarded mental development so low I.Q., delayed puberty; decreased body temperature, heart rate, pulse rate, blood pressure and cardiac output; reduced urine output; decreased sugar level in blood etc. Cretinism can be congenital (absence of thyroid due to genetic defect) or endemic (absence of iodine in diet). It can be corrected by thyroxine administration.
- Myxoedema : It occurs due to deficiency of thyroxine in adults like cretinism, it also has low BMR (by 30 - 40%); low body temperature, reduced heart rate, pulse rate, blood pressure and cardiac output, low sugar and iodine level in blood etc. But the peculiar feature of myxoedema is that face and hands become swollen due to deposition of albuminous myxomatous tissue. It can also be corrected by thyroxine administration. It is also called Gull’s disease.
- Endemic or simple goitre or colloid goitre : It occurs due to deficiency of iodine in drinking water. It is non-genetic (sporadic goitre is a genetic disease) and characterized by enlargement of the thyroid gland due to increase in number and size of acinal cells of the thyroid gland. It is more common in people of hilly region (hence called endemic goiter). To prevent goitre, the table salt is iodised these days.
- Hashimoto's disease : It is called auto-immune thyroiditis and occurs due to age factor, injury-surgery, wrong treatment or injection of thyroid gland causing hypersecretion of thyroxine. When thyroxine secretion falls upto minimal limit, the antibodies are formed which destroy the thyroid gland.
- Exophthalmic goiter (Grave’s disease) : It occurs due to overactivity of the thyroid gland. Exophthalmic goitre is usually accompanied with some asymmetrical protrusion (Exophthalmos) of the eyeballs, imparting an angry, frightened, or staring look to the patient. Protrusion of eyeballs is due to accumulation of mucus in eye orbits.
PARATHYROID GLAND
- Parathyroid glands are present on the back side of the thyroid gland. There are usually 4 parathyroid glands, one pair each in the two lobes of the thyroid gland.
- The parathyroid glands secrete a peptide hormone called parathyroid hormone (PTH) / Collip’s hormone. The secretion of PTH from chief cells is regulated by circulating levels of calcium ions.
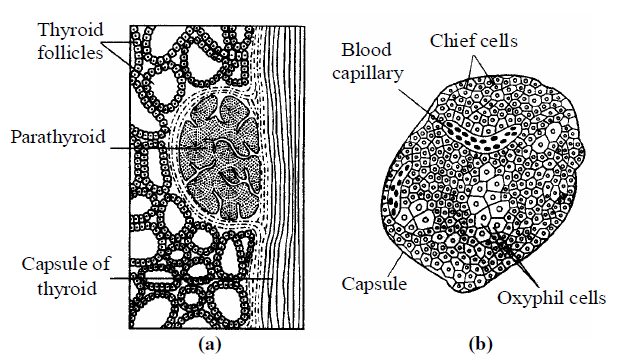
Fig.: (a) Parathyroid gland embedded in the surface of thyroid, (b) Ultrastructure of a parathyroid gland.
- Parathyroid hormone (PTH)
- increases the Ca2+ levels in the blood
- acts on bones and stimulates the process of bone resorption (dissolution/demineralisation)
- also stimulates reabsorption of Ca2+ by the renal tubules and increases Ca2+ absorption from the digested food.
- PTH is a hypercalcemic hormone, i.e., it increases the blood Ca2+ levels. Along with TCT, it plays a significant role in calcium balance in the body.
DISORDERS OF PTH
(1) Hypoparathyroidism (Hyposecretion of parathormone)
- It is rare, however, in under secretion of parathormone, the level of calcium in ECF falls (hypocalcemia), and that of phosphates rises (hyperphosphatemia). This causes neuromuscular hyperexcitability, excessive perspiration, gooseflesh (raising of hairs and prickly sensation in skin), cooling of hands and feet, painful muscular spasms and convulsions, and trembling.
- Sometimes some skeletal muscles, usually of hands and feet, fail to relax after a contraction, and remain in "sustained contraction". This is called "Tetany". Tetany of larygneal, thoracic, and phrenic muscles, which help in breathing, causes death, because the patient fails to breathe (asphyxia).
- Childhood hypoparathyroidism retards growth, particularly of bones, teeth, hair and brain. Vitamin D is administered to such children.
(2) Hyperparathyroidism (Hypersecretion of parathormone)
- Osteoporosis : It occurs usually due to overgrowth of one or more parathyroid glands. It causes demineralization of bones which, therefore, become soft, weak, distorted and fragile. This is called osteoporosis.
- Hypercalcemia : Simultaneously, due to a sharp rise in calcium level in blood and ECF (hypercalcemia) and a sharp fall in phosphate level (hypophosphatemia), muscles and nerves are weakened.
- Hypercalciuria : Calcium is excreted in urine (hypercalciuria), thirst increases owing to copious urination, appetite is lost, constipation and headache become common, and often, kidney stones are formed. The only treatment so far known is removal of extra part of the glands by operation.
THYMUS
- The thymus gland is a lobular structure located on the dorsal side of the heart and the aorta.
- It is the first developing lymphoid organ.
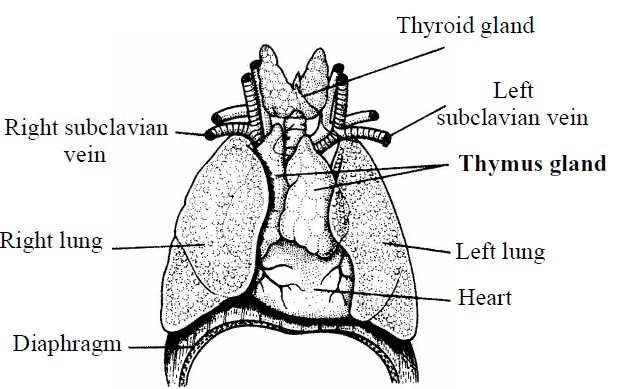
Fig. : Location of thymus gland
- Thymus is divided into two parts - the outer cortex and inner medulla.
- Thymus gland acts as hematopoietic as well as endocrine gland.
- This gland secretes the peptide hormones called thymosin and thymopoietin.
- Thymosin play a major role in the differentiation of T lymphocytes, which provide cell-mediated immunity. In addition, thymosin also promote production of antibodies to provide humoral immunity.
- Thymopoietin (also called thymine I and II) inhibits acetylcholine release at motor release endings.
DISORDER OF THYMUS GLAND
Hypersecretion of thymosin hormone may lead to myasthenia gravis, characterised by abnormal muscular excitation.
ADRENAL GLAND
- Adrenal glands are two small yellowish gland located on superior to kidney (hence called suprarenal gland)
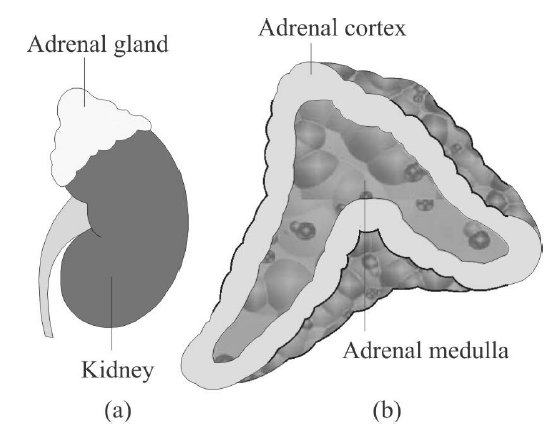
Fig. : Diagrammatic representation of : (a) Adrenal gland above kidney (b) Section showing two parts of adrenal gland
- Each gland is composed of two types of tissues - the centrally located adrenal medulla, and outside this lies the adrenal cortex.
- The adrenal medulla consists of chromaffin cells and secretes two hormones - adrenaline (or epinephrine) and noradrenaline (or norepinephrine). These are commonly called as catecholamines.
- Adrenaline and nor-adrenaline are derived from amino acid tyrosine and are rapidly secreted in response to stress of any kind and during emergency situations. Hence, called emergency hormones or hormones of fight or fright or flight.
- These hormones increase alertness, pupilary dilation, piloerection (raising of hairs), sweating etc. Both the hormones increase the heart beat, the strength of heart contraction and the rate of respiration.
- Catecholamines also stimulate the breakdown of glycogen resulting in an increased concentration of glucose in blood. In addition, they also stimulate the breakdown of lipids and proteins.
- Secretion of adrenaline is 5-10 times higher than nor-adrenaline.
- The adrenal cortex can be divided into three layers - zona reticularis (inner layer), zona fasciculata (middle layer) and zona glomerulosa (outer layer).
- Zona glomerulosa secretes mineralocorticoids primarily aldosterone.
- Zona fasciculata secretes glucocorticoids mainly cortisol.
- Zona reticularis secretes sex corticoids including testosterone.
- The adrenal cortex secretes many steroid hormones, which are commonly called as corticoids. Corticoids, which are involved in carbohydrate metabolism are called glucocorticoids. Cortisol is the main glucocorticoid.
- Glucocorticoids stimulate gluconeogenesis, lipolysis and proteolysis; and inhibit cellular uptake and utilization of amino acids.
- Cortisol maintain the cardiovascular system as well as the kidney functions and produces anti-inflammatory reactions and suppresses the immune response. Cortisol stimulates the RBC production.
- Corticoids, which regulate the balance of water and electrolytes in our body are called mineralocorticoids. Aldosterone is the main mineralocorticoid.
- Aldosterone (also called salt retaining hormone) acts mainly at the renal tubules and stimulates the reabsorption of Na+ and water and excretion of K+ and phosphate ions. Thus, aldosterone helps in the maintenance of electrolytes, body fluid volume, osmotic pressure and blood pressure.
- Small amounts of androgenic steroids are also secreted by the adrenal cortex (Zona reticularis and Zona fasciculata) which play a role in the growth of axial hair, pubic hair and facial hair during puberty.
DISORDERS OF ADRENAL HORMONES
- Hyposecretion : This may be a genetic defect. Under secretion of adrenocorticoids (hypocorticism) causes Addison's disease which is relatively rare and occurs in both men and women between the ages of 20 to 40 years. This disease was first described by Thomas Addison in 1849, 1855. It is maintained in the following symptoms :
- Owing to low aldosterone and glucocorticoids level in blood, considerable amount of sodium ions and water is excreted in urine, leading to dehydration, low blood pressure, and weakness, all symptoms of a peculiar, Addinosonean anaemia which is different from common pernicious anaemia resulting from entirely different causes like diarrhoea, cholera, etc.
- Owing to low cortisol level, glucose level also falls in blood (hypoglycemia). This sharply reduces BMR in body cells. Due to hypoglycemia and hyperkalemia (increased K+ level in blood, efficiency of brain, liver, skeletal and cardiac muscles, etc declines. Body temperature also falls. Heartbeat may even stop causing death.
- Decreased cortisol level induces gastro-intestinal disorders, resulting in loss of appetite, nausea, vomiting, diarrhoea, abdominal pain and restlessness.
- Due to a sharp decline in the body's chemical defense and resistance, sensitivity to cold, heat, infection, poisoning and other adverse condition increases. Acute hypocorticism is catastrophic and threatens life. Complete destruction of removal of adrenals causes death in a short time, principally because of loss of excessive sodium in urine.
- Addison's disease also causes an increase in the number of WBCs, resulting into eosinophilia, lymphocytosis, leukocytosis, etc.
- Undersecretion of sex hormones causes impotence in males and disorders of menstrual cycle in females.
- Excessive deposits of melanin, particularly in the skin of open parts of body like face, hands, feet, neck, teats, etc, cause deep bronzing of skin in these parts.
- An increase in H+ concentration in blood may cause acidosis.
- Pheochromocytoma is due to hypersecretion of adrenaline. It causes, high blood pressure, high level of sugar in blood and urine, high metabolic rate, nervousness and sweating.
- Hypersecretion : Oversecretion of adrenocorticoids (hypercorticism) causes following disorders and diseases -
- Glucose level rises in blood (hyperglycemia). This may lead to diabetes mellitus.
- Irregular deposits of fat, particularly in thoracic parts and face, imparts asymmetrical shape to the body. The face becomes red and rounded (moon face), shoulders swell (buffalo humps) and abdomen dilates and often shows lines of stretching. All these are symptoms of Cushing's disease (Cushing, 1932). Patients may die from brain haemorrhage, cardiac arrest, pneumonia, etc.
- Retention of sodium and water in the ECF increases blood pressure, causing severe hypertension and associated symptoms like severe headache.
- Excessive loss of potassium in urine causes potassium deficiency (hypokalemia). This leads to muscular weakness and convulsions and nervous disorders, and may even cause tetany and paralysis, copious and frequent urination (polyuria) and thirst, bed urination (nocturia), etc. Similarly, excessive loss of H+ in urine may cause alkalosis.
- Hypersecretion (of aldosterone) due to adrenal cortical tumor lead to conn’s syndrome. It is also called aldosteronism. It is characterized by rise in blood volume and blood pressure but without Oedema, muscular weakness, high Na+ and low K+ level in blood plasma resulting in kidney damage with polyuria and tetany and metabolic disorder.
- Excessive secretion of sex corticoids (androgen) due to tumor of adrenal cortex result in Virilism and hirsutism in female and gynaecomastia in male.
- Virilism is appearance of male secondary characters like male voice beard, moustache, stoppage of menstruation and growth of clitoris in females.
- Hirsutism is the presence of facial and excess body hair in females.
- Gynaecomastia is characterized by enlarged mammary gland.
PANCREAS
- Pancreas is located within the curve of the duodenum. It is the second largest gland of the body.
- Pancreas is a heterocrine gland as it has both exocrine and endocrine tissues.
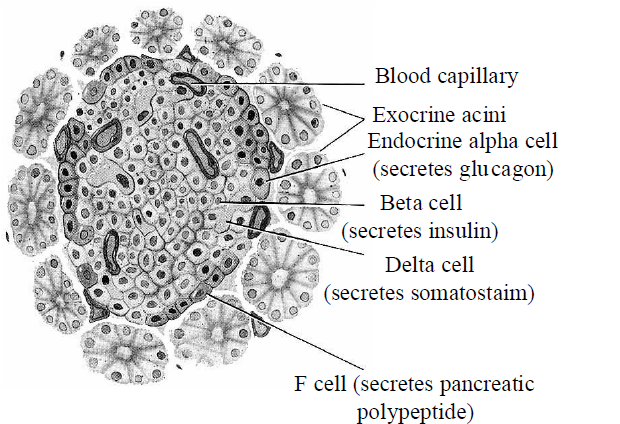
Fig.: T.S. of pancreas
- The exocrine part occurs as acini and endocrine pancreas consists of ‘Islets of Langerhans’.
- Hormones secreting cells present in Islet of Langerhans are given in the table below.

- Glucagon is a peptide hormone and plays an important role in maintaining the normal blood glucose levels. It acts mainly on the liver cells (hepatocytes) and stimulates glycogenolysis resulting in an increased blood sugar (hyperglycemia).
- Glucagon reduces the cellular glucose uptake and utilization. Thus, glucagon is a hyperglycemic hormone.
- Insulin is a peptide hormone, which plays a major role in the regulation of glucose homeostasis. Insulin acts mainly on hepatocytes and adipocytes (cells of adipose tissue), and enhances cellular glucose uptake and utilization.
- Insulin also stimulates the conversion of glucose to glycogen (glycogenesis) in the target cells.
- Normal range of blood sugar is 80-120 mg/100 ml of blood.
- Gastrin is similar to the one produced by pyloric stomach
- Somatostatin controls α and β cells of the pancreas.
- Pancreatic polypeptide check secretory activity of digestive glands and increases glycogenolysis.
DISORDERS OF PANCREAS
- Hyposecretion leads to diabetes mellitus, which is associated with loss of glucose through urine and formation of harmful compounds known as ketone bodies.
- It occurs due to either deficient insulin production or due to failure of cells to take up insulin from blood. It is characterized by hyperglycemia (300-1200 mg/100 ml), polyciria (excessive urination due to increase in water content in urine), polydipsia (excessive thirst), glycosuria (glucose in urine), loss of weight and tiredness, dehydration, reduced healing power etc.
TESTIS
- Testis is present in the scrotal sac (outside abdomen) of male individuals.
- Testis performs dual functions as a primary sex organ as well as an endocrine gland.
- Testis is composed of seminiferous tubules and stromal or interstitial tissue.
- The Leydig cells or interstitial cells, present in the intertubular spaces produce a group of hormones called androgens (mainly testosterone).
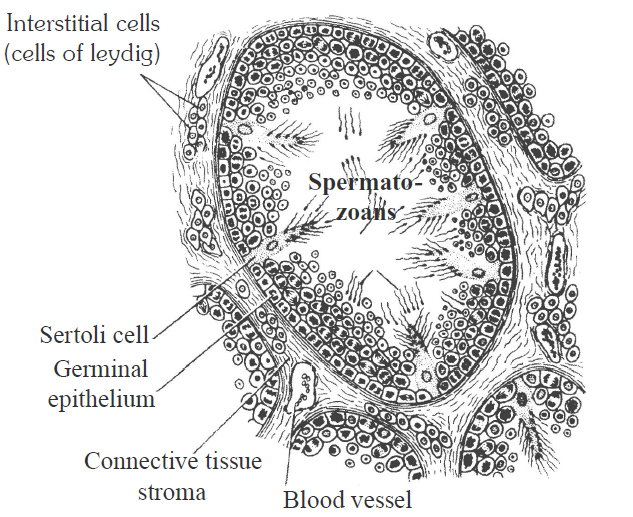
Fig.: Testes
- Androgens regulate the development, maturation and functions of the male accessory sex organs like epididymis, vas deferens, seminal vesicles, prostate gland, urethra etc. These hormones stimulate muscular growth, growth of facial and axillary hair, aggressiveness, low pitch of voice etc.
- Androgens play a major stimulatory role in the process of spermatogenesis (formation of spermatozoa). Androgens act on the central neural system and influence the male sexual behaviour (libido). These hormones produce anabolic (synthetic) effects on protein and carbohydrate metabolism.
- Failure of testosterone secretion in male-causes eunuchoidism. Eunuch has a undeveloped secondary sex organs like prostrate, seminal vesicle and penis and they does not produce sperm.
OVARY
- Ovary is the primary female sex organ which lies in the abdominal cavity.
- It produces one ovum during each menstrual cycle and also produces two groups of steroid hormones called estrogen and progesterone.

Fig. : Ovary
- Ovary is composed of ovarian follicles and stromal tissues. It secretes estrogen and progesterone.
- The estrogen is synthesized and secreted mainly by the growing ovarian follicles. After ovulation, the ruptured follicle is converted to a structure called corpus luteum, which secretes mainly progesterone.
- Estrogens produce wide ranging actions such as stimulation of growth and activities of female secondary sex organs, development of growing ovarian follicles, appearance of female secondary sex characters (e.g., high pitch of voice, etc.), mammary gland development.
- Progesterone supports pregnancy and also acts on the mammary glands and stimulates the formation of alveoli (sac-like structures which store milk) and milk secretion.
HORMONES OF HEART, KIDNEY AND GASTROINTESTINAL TRACT
- The atrial wall of heart secretes a very important peptide hormone called atrial natriuretic factor (ANF), which decreases blood pressure. When blood pressure is increased, ANF is secreted which causes dilation of the blood vessels. This reduces the blood pressure.
- The juxtaglomerular cells of the kidney produce a peptide hormone called erythropoietin which stimulates erythropoiesis (formation of RBC).
- Endocrine cells present in different parts of the gastro-intestinal tract secrete four major peptide hormones, namely gastrin, secretin, cholecystokinin (CCK) and gastric inhibitory peptide (GIP).
- Gastrin acts on the gastric glands and stimulates the secretion of hydrochloric acid and pepsinogen.
- Secretin acts on the exocrine pancreas and stimulates secretion of water and bicarbonate ions.
- CCK acts on both pancreas and gallbladder and stimulates the secretion of pancreatic enzymes and bile juice, respectively.
- GIP inhibits gastric secretion and motility.
CLASSIFICATION OF HORMONES
ON THE BASIS OF CHEMICAL NATURE
- On the basis of chemical composition, hormones are classified into three categories – amine hormones, steroids, proteinaceous and peptide hormones.
- Amine hormones are derived from tyrosine amino acid and have amino group, e.g., thyroxine, epinephrine, nor-epinephrine.
- Steroids are fat soluble and have sterol group. These are derived from cholesterol, e.g., hormones of adrenal cortex (cortisol, cortisone, corticosterone, aldosterone), testes (testosterone) and ovaries (estrone, estradiol, progesterone etc.)
- Proteinaceous and peptide hormones are formed of 3-200 amino acids interlinked by peptide bonds and are water soluble. E.g.,
- Proteinaceous hormones like STH, TSH, FSH, LH etc. Out of these, FSH and LH are glycoproteins.
- Long peptide hormones like insulin and glucagon, ACTH, parathormone.
- Short peptide hormones like oxytocin, ADH, MSH. These hormones are formed of a few amino acids.
ON THE BASIS OF MODE OF ACTION
- On the basis of mode of action, hormones are of two types – quick acting hormones and delayed acting hormones.
- Quick acting hormones : These hormones initiate immediate response from their target cells. Their receptor is always located on the outer surface of the plasma membrane of target cell because these are large sized. Hormone receptor complex activates a membrane enzyme-adenylyl cyclase which hydrolyse ATP into cyclic AMP, which acts as secondary messenger. c-AMP activates an inactive enzyme system by cascade effect. So, their mode of action is called second messenger hypothesis. E.g., proteinaceous, peptide and amine hormones.
- Delayed acting hormones : These hormones initiate response after sometime. These are small sized so are diffusible through the plasma membrane of their target cell. These bind their proteinaceous receptor present in the cytosol. These always operate through de-novo synthesis of m-RNA by activation of certain genes. So, their mechanism of action is called m-RNA hypothesis. E.g., steroid hormones of testes, ovary and adrenal cortex.
MECHANISM OF HORMONE ACTION
- Hormones produce their effects on target tissues by binding to specific proteins called hormone receptors located in the target tissues only.
- Each receptor is specific to one hormone only and hence receptors are specific.
- Hormone-receptor complex formation leads to certain biochemical changes in the target tissue. Target tissue metabolism and hence physiological functions are regulated by hormones.
- Hormones which interact with intracellular receptors (e.g., steroid hormones, iodothyronines, etc.) mostly regulate gene expression or chromosome function by the interaction of hormone-receptor complex with the genome.
- The hormone receptor complex may act in one of the two ways - formation of cAMP and change in membrane permeability.
(1) Formation of cAMP
The hormone receptor complex causes the release of an enzyme adenyl cyclase, from the receptor site. This enzyme hydrolyses the ATP into c-AMP. The c-AMP activates the existing enzyme system of the cell. This accelerates the metabolic reactions in the cell.
The hormone is called first messenger and the c-AMP is termed theb. E.g., Adrenaline causes the secretion of glucose from the liver cell from this mechanism.
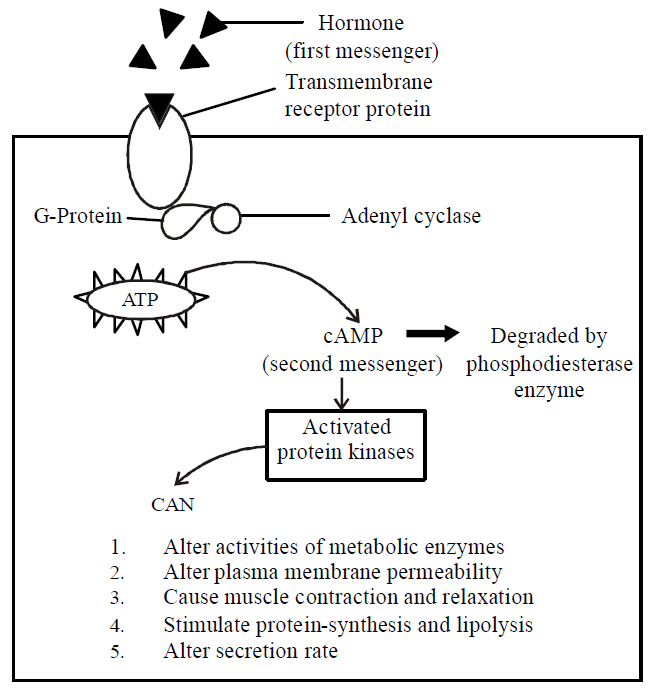
Fig. : Mechanism of hormone action on cell surface
(2) Change in membrane permeability
- The receptor proteins of some hormones are large transmembrane intrinsic protein acting as ion channels for facilitated diffusion of Na+, K+, Ca2+ etc. On binding with specific hormone, these receptor proteins undergo conformational changes, so that the membrane permeability for ions is altered, resulting into important changes in metabolism.
- For example, insulin promotes the entry of glucose from blood into the muscles cells by increasing the permeability of sarcolemma to glucose.
- The steroid hormones act within the cell. Their small, lipid soluble molecules pass through the cell membrane and bind to specific receptor molecules present in the cytoplasm. The receptor molecules carry them into the nucleus. Here, the receptor hormone complex binds to a specific receptor site on the chromosome and activates certain genes that were previously repressed. The activated gene transcribe m-RNA which directs the synthesis of enzyme (protein molecule) in the cytoplasm. The enzyme molecule promote the metabolic reactions in the cell.
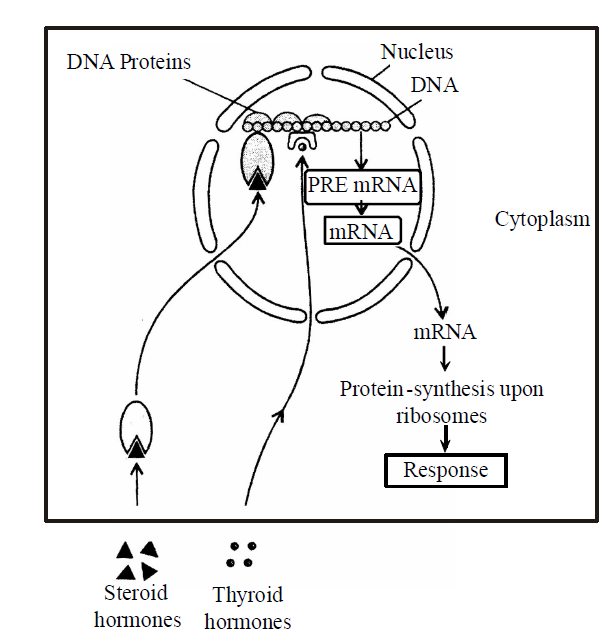
Fig. : Mechanism of hormone action within a cell
Table : Hormones, their chemical nature and functions at a glance.
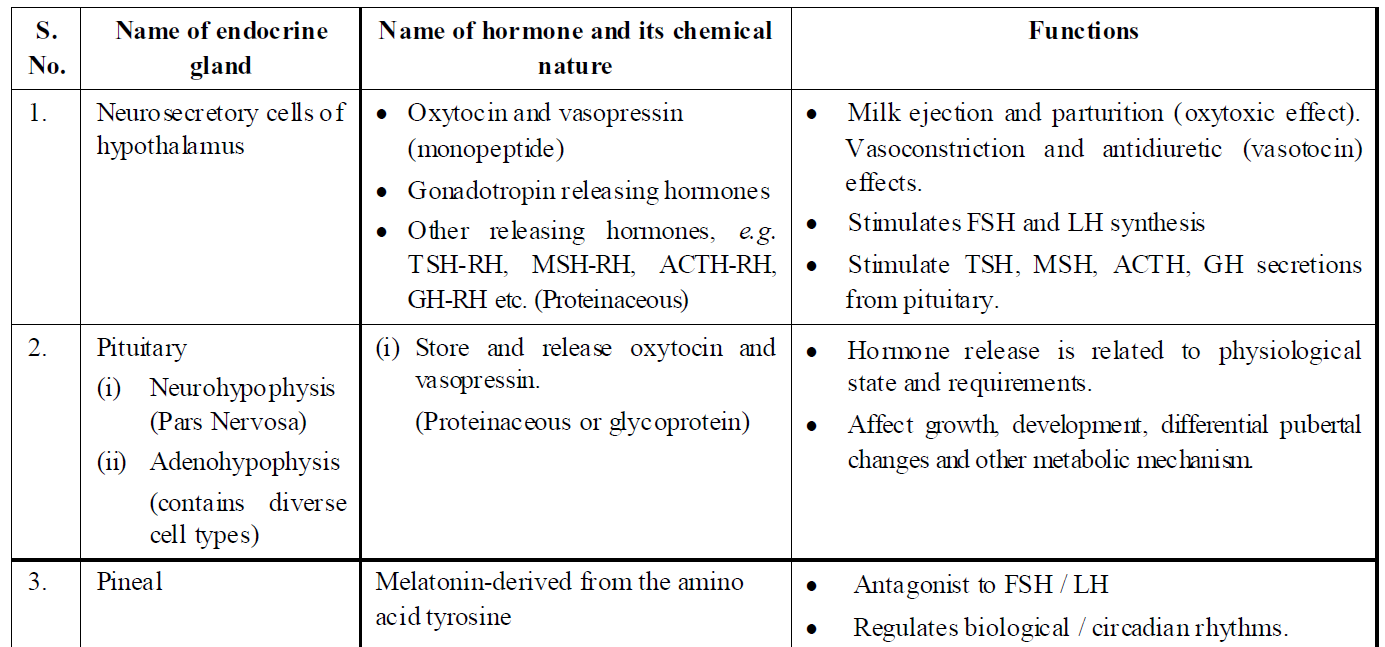
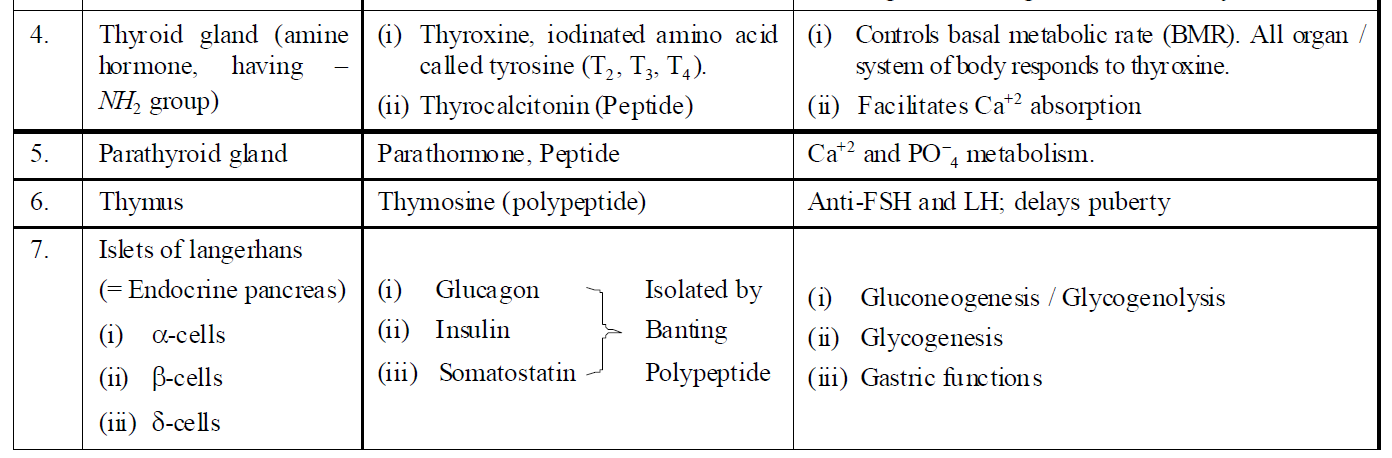
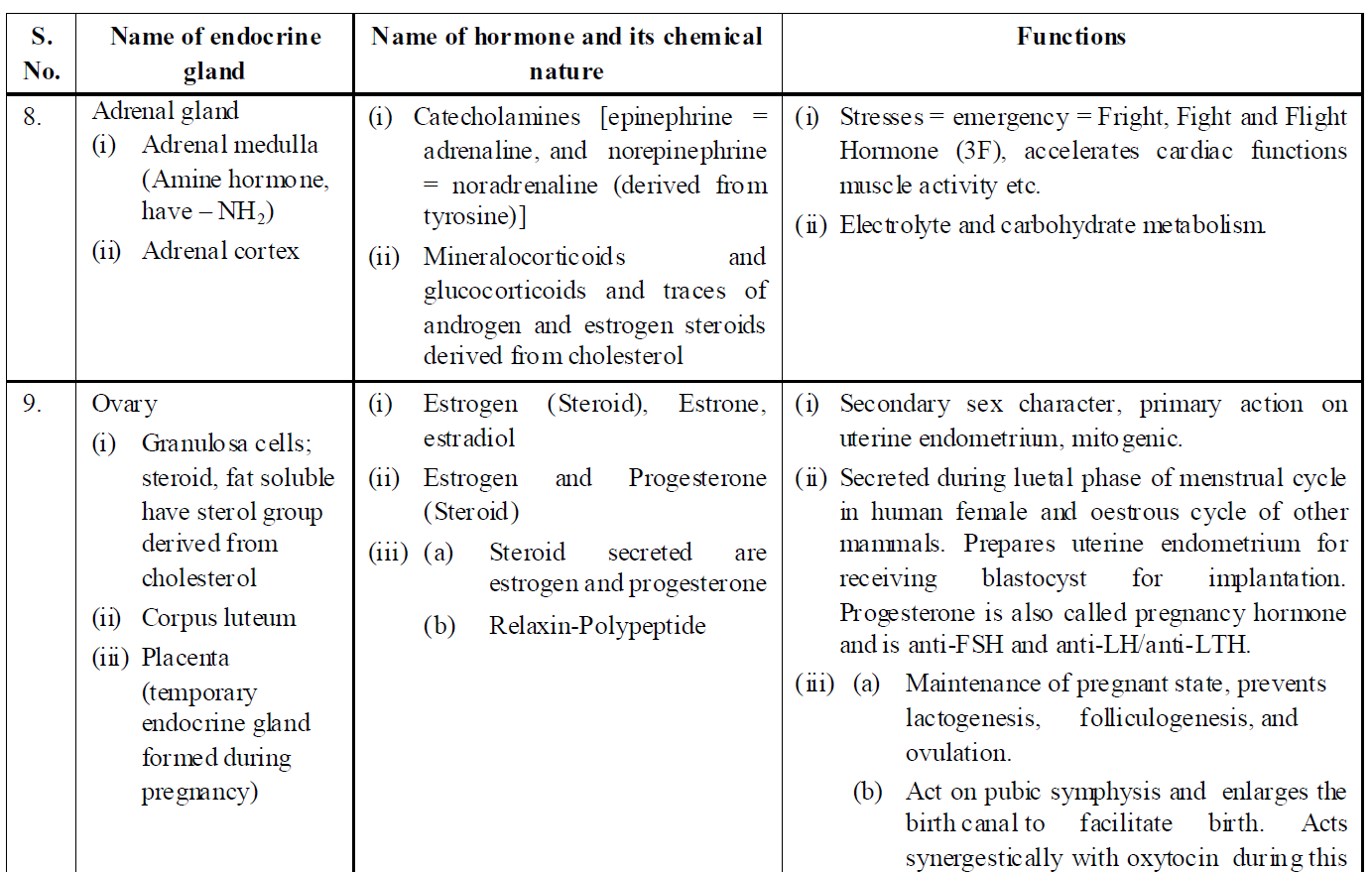
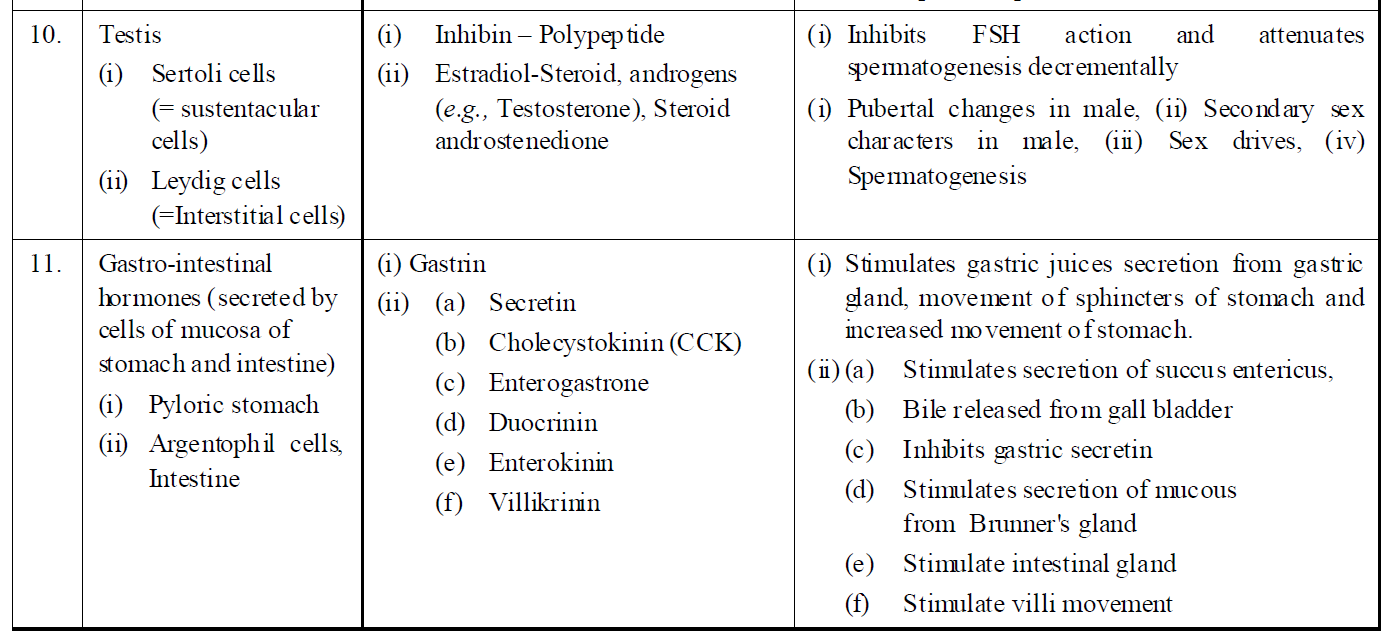
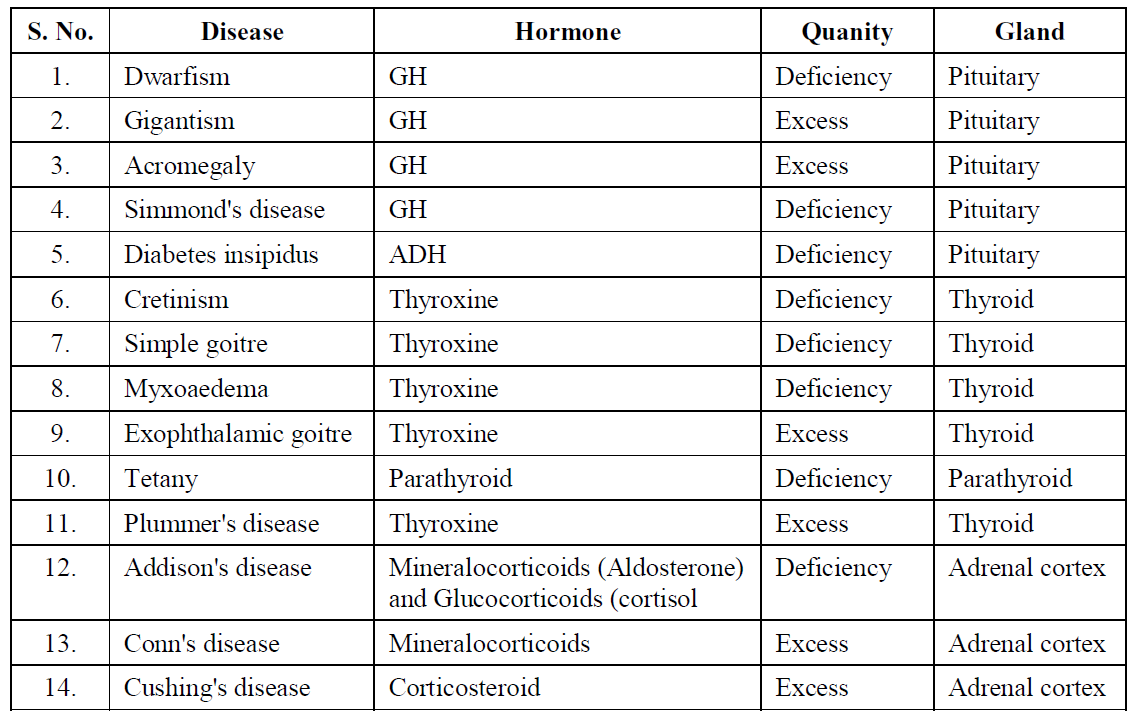
Table : Disease caused by hormonal irregularities
Post a Comment