
BREATHING AND EXCHANGE OF GASES
INTRODUCTION
- Respiration is the involuntary catabolic process which involves exchange of environmental oxygen and body's carbon dioxide. The oxygen is utilized for the oxidation of glucose in the mitochondria to produce energy.
- It takes place in three basic steps -
- Pulmonary ventilation : The first process, pulmonary (pulmo = lung) ventilation, or breathing, is the inspiration (inflow) and expiration (outflow) of air between the atmosphere and lungs.
- External (pulmonary) respiration : This is the exchange of gases between air spaces of the lungs and blood in pulmonary capillaries. The blood gains O2 and loses CO2.
- Internal (tissue) respiration : The exchange of gases between blood in systemic capillaries and tissue cells is known as internal (tissue) respiration. The blood loses O2 and gains CO2 within cells. The metabolic reactions that consume O2 and give off CO2 during production of ATP are termed as cellular respiration.
- Respiration is of two types – aerobic and anaerobic respiration.
- Aerobic respiration occurs in the presence of molecular oxygen. The oxygen completely oxidizes the food to carbon dioxide and water releasing large amounts of energy.
- The organisms showing aerobic respiration, are called aerobes. It is found in most animals and plants.
- Aerobic respiration are of two main types – direct and indirect.
- Direct respiration is the exchange of environmental oxygen with carbon dioxide of the body cells without special respiratory organs and without the aid of blood. It is found in aerobic bacteria, protists, plants, sponges, coelenterates, flatworms, roundworms and most arthropods.
- Indirect respiration involves special respiratory organs such as skin, buccopharyngeal lining, gills and lungs and needs the help of blood. Respiration in the skin, buccopharyngeal lining, gills and lungs is respectively called cutaneous, buccopharyngeal, bronchial and pulmonary respiration.
- Cutaneous respiration takes place in annelids, some crustaceans, eel fish, amphibians and marine snakes. It occurs both in water and in air.
- Buccopharyngeal respiration is found in certain amphibians such as frog and toad. It occurs in the air.
- Bronchial respiration is found in many annelids, most crustaceans and molluscs, some insect larvae, echinoderms, all fishes and some amphibians. It occurs in water only.
- Pulmonary respiration is found in snails, Pila, some amphibians and reptiles, birds and mammals. It takes place in air only.
- Anaerobic respiration occurs in the absence of molecular oxygen and is also called fermentation. In this, the food is partially oxidized so only a part of energy (5%) is released and some of the energy remains trapped in the intermediate compounds. It is found in lower organisms like bacteria and yeast. It is also found in certain parasitic worms (Ascaris, Taenia) which live in deficient medium.
- For efficient gas exchange, the respiratory membrane, through which exchange of gases takes place should have the following qualities.
- It should be thin, large and moist.
- It should be completely permeable for O2 and CO2.
- It should have high vascularity (rich blood supply).
- Its surface area should be very large
- Presence of respiratory pigments (e.g., haemoglobin) in many animals to increase the O2 and CO2 carrying capacity of the blood.
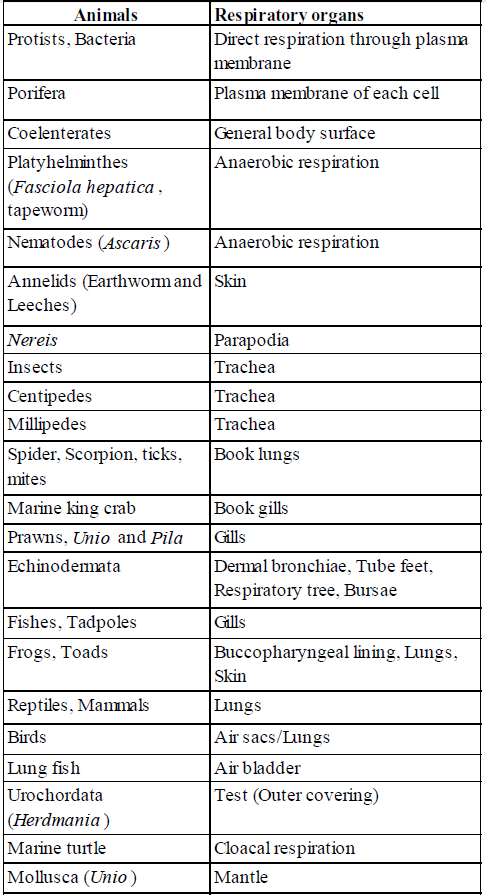
Table : Types of respiration and respiratory organs of animals
RESPIRATORY SYSTEM IN HUMANS
- Respiratory system is endodermal in origin.
- Respiratory system is composed of conducting portion and a respiratory portion.
- The conducting portion provides a passage way for air and functions to condition the incoming air by warming, moistening and cleaning it. It consists of nasopharynx, larynx, trachea, bronchi, bronchioles and terminal bronchioles.
- The respiratory portion consisting of bronchioles, alveolar ducts and alveolar sacs serves to get rid the body of CO2 and pick up oxygen.
- A pair of external nostrils leads to a nasal chamber through the nasal passage.
- The nasal chamber opens into nasopharynx which is a portion of pharynx, the common passage for food and air.
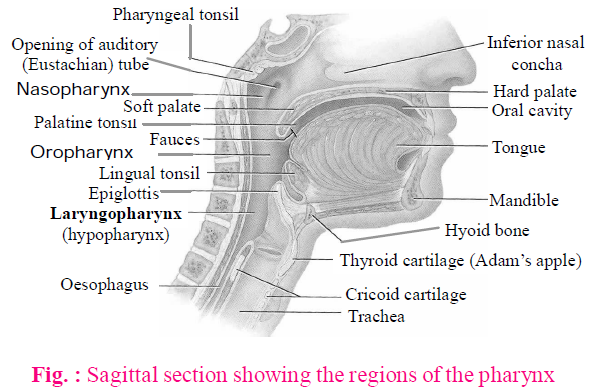
- Nasopharynx opens through glottis of the larynx region into the trachea.
- Larynx is composed of cartilages, ligaments, muscles and a mucosal surface. It helps in sound production and hence called the sound box.
- It prevents indigested solids and liquids from entering the respiratory system.
- Larynx is also called Adam's apple in human males.
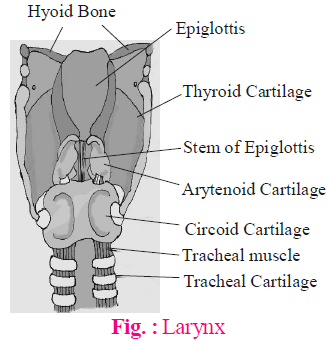
- During swallowing, glottis can be covered by a thin elastic cartilaginous flap called epiglottis to prevent the entry of food into the larynx.
- Besides epiglottis, other cartilages of the larynx are – thyroid cartilage (most prominent C– shaped), cricoid cartilage (shape like a signet ring) and arytenoid cartilage (at the anterior of which cartilage of Santorinis is attached).
- Trachea windpipe is a straight tube extending up to the mid-thoracic cavity, which divides at the level of 5th thoracic vertebra into a right and left primary bronchi.
- Trachea carries air between the larynx and bronchi and is supported by incomplete rings of C-shaped cartilage (hyoid bone) in its wall.
- The rings of cartilage makes the wall non-collapsible.
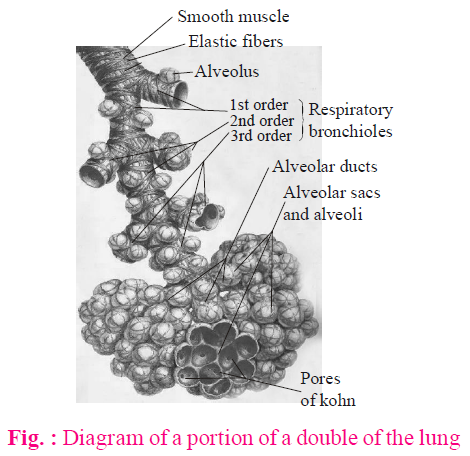
- Each bronchi undergoes repeated divisions to form the secondary and tertiary bronchi and bronchioles ending up in very thin terminal bronchioles.
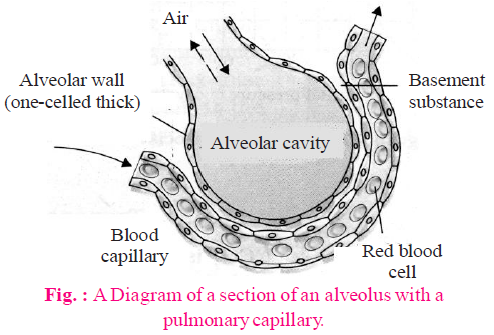
- Each terminal bronchiole gives rise to a number of very thin, irregular walled and vascularised bag-like structures called alveoli.
- Alveoli (made of simple squamous cells) provides a huge surface area for gaseous exchange.
- Alveoli is surrounded by a network of capillaries of the pulmonary artery and veins.
- Air enters into the lung in this way -
Inhaled air  Mouth/Nose, or nasal chamber
Mouth/Nose, or nasal chamber  Larynx
Larynx  Glottis
Glottis Trachea
Trachea Right and left bronchi
Right and left bronchi  Bronchioles
Bronchioles Alveoli
Alveoli
- Number of alveoli is 300-400 million with a surface area of 100 sq.m.
- Surfactant is a lipid surface tension lowering agent which prevents alveoli from collapsing during respiration.
- The branching network of bronchi, bronchioles and alveoli comprise the lungs.
- Lung is the primary respiratory organ.
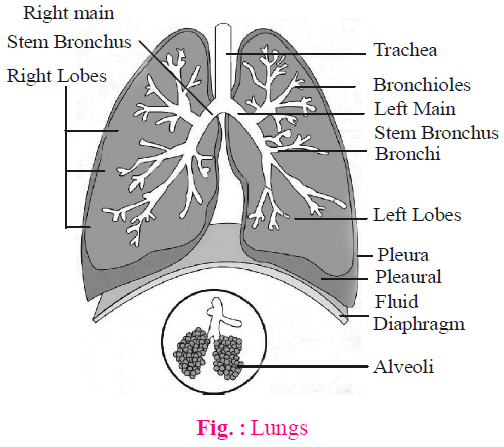
- Lungs are covered by a double layered pleura, with pleural fluid between them. It reduces friction on the lung surface. The outer pleural membrane (visceral pleural membrane) is in close contact with the thoracic lining whereas the inner pleural membrane (parietal pleural membrane) is in contact with the lung surface.
- A small space called mediastinum lies in between the two lungs.
- The right lung is divided into three lobes and the left lung into two lobes.
- The left lung is smaller than the right lung.
- The anatomical setup of lungs in thorax is such that any change in the volume of the thoracic cavity will be reflected in the lung (pulmonary) cavity. Such an arrangement is essential for breathing, as we cannot directly alter the pulmonary volume.
- Diaphragm is a highly muscular and fibrous dome shaped muscle.
- Important function of diaphragm is to aid in respiration. It separates the thoracic and abdominal cavities. It is also called phrenic muscles.
- The contraction of diaphragm assists in inspiration, micturition, defecation and parturition.
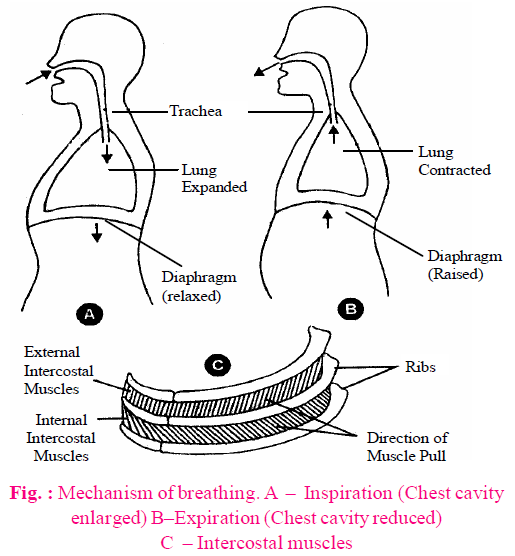
MECHANISM OF BREATHING
- Breathing involves two phases : inspiration (during which atmospheric air is drawn in) and expiration (by which the alveolar air is released out).
- The movement of air into and out of the lungs is carried out by creating a pressure gradient between the lungs and the atmosphere.
- Inspiration can occur if the pressure within the lungs (intrapulmonary pressure) is less than the atmospheric pressure, i.e., there is a negative pressure in the lungs with respect to atmospheric pressure. Similarly, expiration takes place when the intrapulmonary pressure is higher than the atmospheric pressure.
- Respiration is carried out with the help of intercostal muscles and diaphragm. Intercostal muscles, between each pair of ribs, are of two types- external and internal.
- Inspiration is an active process and involves internal intercostal muscles and diaphragm.
- During inspiration, contraction of diaphragm increases the volume of thoracic chamber in the antero-posterior axis. The contraction of external intercostal muscles lifts up the ribs and the sternum causing an increase in the volume of the thoracic chamber in the dorso-ventral axis. The overall increase in the thoracic volume causes a similar increase in pulmonary volume. An increase in pulmonary volume decreases the intrapulmonary pressure to less than the atmospheric pressure which forces the air from outside to move into the lungs, i.e., inspiration.
- Expiration is a passive process and caused due to muscle relaxation.
- Relaxation of the diaphragm and the intercostal muscles returns the diaphragm and sternum to their normal positions and reduce the thoracic volume and thereby the pulmonary volume. This leads to an increase in intrapulmonary pressure to slightly above the atmospheric pressure causing the expulsion of air from the lungs, i.e., expiration.
- During deep or forced breathing or heavy exercise, an active process is involved requiring internal intercostal muscles and diaphragm.
- Deep expiration is done by contraction of internal intercostal muscles and relaxation of other muscles and diaphragm. Impulse for deep breath starts from cerebrum.
- The deep breathing is referred to as thoracic breathing in contrast to the normal or quiet breathing referred to as abdominal breathing.
- Sudden deep breath is due to increased pCO2 and decreased pO2.
- Breathing at high altitude : Air at mountains is thin and of low density. Residents of high altitudes are acclimatized. Visitors first suffer from hypoxia (at 4000 m). This causes mountain sickness including high blood pressure and high breathing rate (normal rate of breathing is 12 to 18/minute). Visitor becomes normal after some days when his number of RBC, and haemoglobin percentage increases.
- Inspiration is for about 2 seconds and expiration for 3 seconds.
- Dead space encloses the air not involved in gaseous exchange as it is enclosed in the respiratory passage such as nasal chamber. It reduces the amount of fresh air that enters the lungs.
- Cough is the forcible expiration usually preceded by a prolonged inspiration.
- Rate of breathing is
- 40 - 60/min in neonates,
- 14 - 18/min in adolescents,
- 12 - 14/min in human adults
- 18 - 22 /min in children.
- 0 in embryo
- 10/min (minimum) at the time of sleeping
- 80/min in frog
- 38/min in rabbit
- 120/min (maximum) in shrew
- 6/min in elephant
- On an average, a healthy human breathes 12-16 times/minute.
RESPIRATORY VOLUMES
Respiratory (Pulmonary) volume is the volume of air in the lungs.
It is of the following types –
It is of the following types –
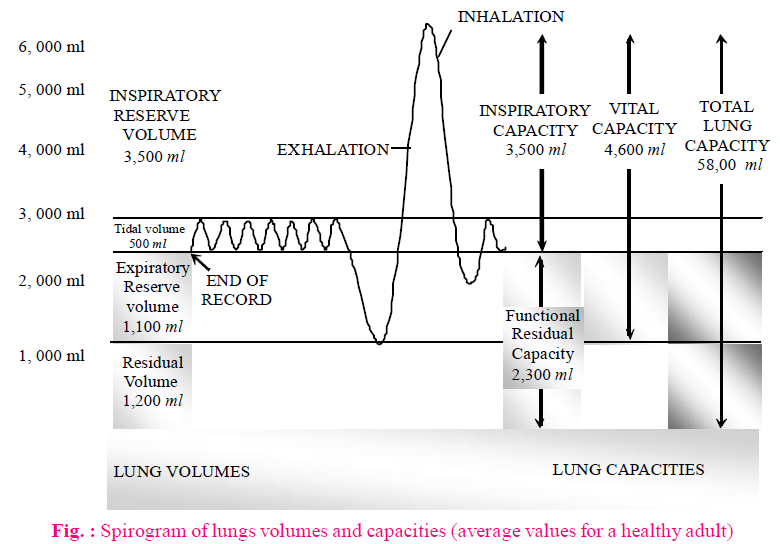
- Tidal Volume (TV) : It is the volume of air inspired or expired during a normal respiration. It is approx. 500 ml., i.e., a healthy man can inspire or expire approximately 6000 to 8000 ml of air per minute.
- Inspiratory Reserve Volume (IRV) : The maximum volume of air, a person can inspire by a forcible inspiration over and above the tidal volume. This averages 2500 ml to 3000 ml.
- Expiratory Reserve Volume (ERV) : It is the additional volume of air, a person can expire by a forcible expiration. This averages 1000 ml to 1100 ml.
- Residual Volume (RV) : The volume of air left in the lungs even after a maximum forcible expiration. This averages 1100 ml to 1200 ml.
RESPIRATORY CAPACITIES
Pulmonary capacities is the combination of two or more pulmonary volumes.
It could be -
It could be -
- Inspiratory Capacity (IC) : It is the total volume of air a person can inspire after a normal expiration. It includes tidal volume and inspiratory reserve volume ( TV+IRV). It is about 3500 ml.
- Expiratory Capacity (EC) : Total volume of air a person can expire after a normal inspiration. This includes tidal volume and expiratory reserve volume (TV+ERV).
- Functional Residual Capacity (FRC) : It is the total volume of air that will remain in the lungs after a normal expiration. This includes ERV+RV. It is about 2300 ml.
- Vital Capacity (VC) : It is the maximum volume of air a person can breathe in after a forced expiration. This includes ERV, TV and IRV or the maximum volume of air a person can breathe out after a forced inspiration. It is about 4600 ml.
- Total Lung Capacity : It is the total volume of air accommodated in the lungs at the end of a forced inspiration. This includes RV, ERV, TV and IRV or vital capacity + residual volume of air. It is about 5800 ml.
EXCHANGE OF GASES
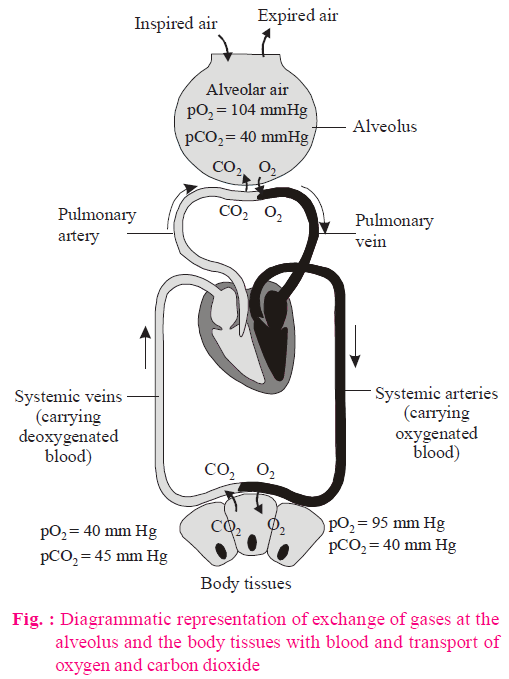
- Alveoli are the primary sites of exchange of gases.
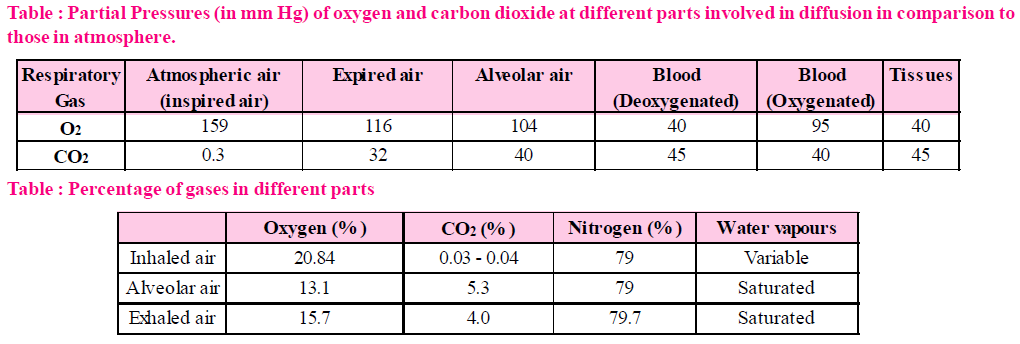
- The exchange of gases between the alveoli and blood in lungs and between the blood and tissue is the result of differences in partial pressure of the respiratory gases i.e., oxygen, carbon dioxide and nitrogen etc.
- O2 and CO2 are exchanged in these sites by simple diffusion mainly based on pressure/concentration gradient.
- Solubility of the gases as well as the thickness of the membranes involved in diffusion can affect the rate of diffusion.
- A concentration gradient is present for oxygen from the alveoli to blood and blood to tissues. Similarly, direction, i.e., from tissues to blood and blood to alveoli is for CO2. As the solubility of CO2 is 20-25 times higher than that of O2, the amount of CO2 that can diffuse through the diffusion membrane per unit difference in partial pressure is much higher compared to that of O2.
- The diffusion membrane is made up of three major layers, the thin squamous epithelium of alveoli, the endothelium of alveolar capillaries and the basement substance in between them.
- All the factors in our body are favourable for diffusion of O2 from alveoli to tissues and that of CO2 from tissues to alveoli.
TRANSPORT OF GASES
Blood is the medium of transport for O2 and CO2.
TRANSPORT OF OXYGEN
- Oxygen is transported in the blood in two ways -
- by mixing with haemoglobin (97%) as oxyhaemoglobin.
- by dissolving in plasma (3%).
- Haemoglobin is a red coloured iron containing pigment present in the RBCs.
- Each haemoglobin molecule can carry a maximum of four molecules of O2 and can bind with 4 molecules of O2 and hence it is called as oxyhaemoglobin.
- Binding of oxygen with haemoglobin is primarily related to partial pressure of O2.
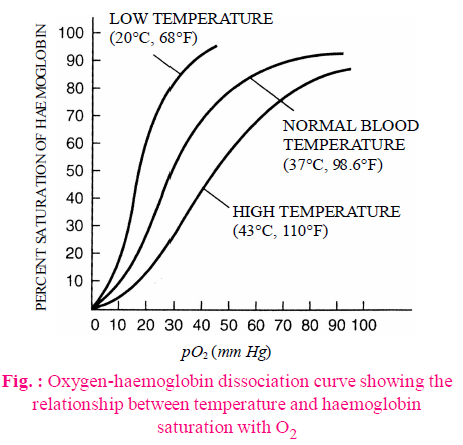
- Partial pressure of CO2, hydrogen ion concentration and temperature are the other factors which can interfere with this binding.
- A sigmoid curve is obtained when percentage saturation of haemoglobin with O2 is plotted against the pO2. This curve is called the oxygen dissociation curve and is highly useful in studying the effect of factors like pCO2, H+ concentration, etc., on binding of O2 with haemoglobin. The percentage of haemoglobin that is bound with oxygen is called percent saturation of haemoglobin.
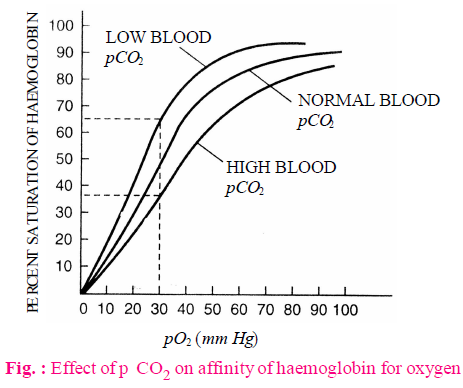
- Bohr's effect refers to the displacement of Hb-O2 dissociation curve to the right and the subsequent increase in P50 that is caused when CO2 tension in blood is high. Bohr discovered this effect in 1904. Bohr effect is the effect of CO2 on oxyhaemoglobin. Deoxygenation of oxyhae-moglobin is directly proportional to blood pCO2. Extent of Bohr's effect depends upon the tension of CO2 in blood only, CO2 of tissue fluid and alveoli does not exert Bohr's effect.
- During exercise, muscles need more O2 and want to remove CO2 which is higher produced. Because of pressure gradient CO2 moves from tissues fluid to capillary blood → exert Bohr's effect → O2 release is hastened from Hb-O2 i.e. Hb-O2 curve shifts to the right.
- In the alveoli, where there is high pO2, low pCO2, lesser H+ concentration and lower temperature, the factors are all favourable for the formation of oxyhaemoglobin, whereas in the tissues, where low pO2, high pCO2, high H+ concentration and higher temperature exists, the conditions are favourable for dissociation of oxygen from the oxyhaemoglobin. This clearly indicates that O2 gets bound to haemoglobin in the lung surface and gets dissociated at the tissues.
- Every 100 ml of oxygenated blood can deliver around 5 ml of O2 to the tissues under normal physiological conditions.
P50 value is the value of PO2 at which haemoglobin is 50% saturated with oxygen to form oxyhaemoglobin.
TRANSPORT OF CARBON DIOXIDE
- Transport of CO2 by blood is much easier than that of oxygen due to high solubility of CO2 in water (about 20 times that of O2)
- Each decilitre of blood carries about 3.7 ml of CO2.
- Carbon dioxide is transported in blood in three ways–
- 7% dissolved in plasma (as carbonic acid)
- 23% bound to haemoglobin (as carbamino-haemoglobin)
- 70% as bicarbonate in the plasma following an enzyme catalyzed reaction in red blood cell.
- RBCs contain a very high concentration of the enzyme, carbonic anhydrase and minute quantities of the same is present in the plasma too. This enzyme facilitates the following reaction in both directions.
CO2 + H2O  H2CO3
H2CO3  HCO3–+H+
HCO3–+H+
- At the tissue site, where partial pressure of pCO2 is high due to catabolism, CO2 diffuses into blood (RBCs and plasma) and forms HCO3– and H+.
- At the alveolar site where pCO2 is low, the reaction proceeds in the opposite direction leading to the formation of CO2 and H2O.
- CO2 trapped as bicarbonate at the tissue level and transported to the alveoli is released out as CO2.
- Every 100 ml of deoxygenated blood delivers approximately 4 ml of CO2 to the alveoli.
- To maintain electrostatic neutrality of plasma, many chloride ions diffuse from plasma into RBC and carbonate ions from RBC to plasma. The chloride content of RBC increases when oxygenated blood becomes deoxygenated is called chloride shift or Hamburger shift. Because of it, the Cl– content of the red blood cells in venous blood is therefore, significantly greater than in arterial blood. The chloride shifts occurs rapidly and is essentially complete in 1 second.
- Haldane effect is the promotion of CO2 dissociation by oxygenation of haemoglobin. It is based on the simple fact that oxyhaemoglobin behaves as strong acid and releases an excess of H+ ions which bind with bicarbonate (HCO3–) ions to form H2CO3 which dissociates into H2O and CO2. Secondly, due to increased acidity CO2 loses the power to combine with haemoglobin and form carbamino haemoglobin.
REGULATION OF RESPIRATION
- Breathing can be controlled by central nervous system.
- Respiratory centres are located in medulla oblongata and pons varolii. These centres regulate the rate and depth of breathing by controlling contraction of diaphragm and other respiratory muscles.
- Medulla oblongata contains inspiratory centre in dorsal portion and expiratory centre in the ventral portion. The expiratory centre is connected with the vagus nerve that innervates the lungs.
- Pons varollii contains pneumotaxic and apneustic centre.
- Pneumotaxic centre can moderate the functions of the respiratory rhythm centre. Neural signal from this centre can reduce the duration of inspiration and thereby alter the respiratory rate. Apneustic centre operates in association with the depth of the inspiration.
- A chemosensitive area situated near rhythm centre is highly sensitive to CO2 and hydrogen ions. Increase in these substances can activate this centre, which in turn can signal the rhythm centre to make necessary adjustments in the respiratory process by which these substances can be eliminated.
- Receptors associated with aortic arch and carotid artery also can recognise changes in CO2 and H+ concentration and send necessary signals to the rhythm centre for remedial actions.
- The role of oxygen in the regulation of respiratory rhythm is quite insignificant.
DISORDERS OF RESPIRATORY SYSTEM
- Asthma is an allergic reaction that causes constriction of the bronchial muscles, thereby reducing the air passage thus, the amount of air that can get to the alveoli.
- Emphysema is a situation of short breath in which alveolar walls are damaged due to which respiratory surface is decreased. It is often caused by cigarette smoking.
- Occupational respiratory disorders : In certain industries, especially those involving grinding or stone-breaking, so much dust is produced that the defense mechanism of the body cannot fully cope with the situation. Long exposure can give rise to inflammation leading to fibrosis (proliferation of fibrous tissues) and thus, causing serious lung damage.
- Hypoxia is a condition of oxygen shortage in the tissues. It is of two types :
- Artificial hypoxia : It results from shortage of oxygen in the air at high (over 2400 m) altitudes. It causes mountain sickness characterized by breathlessness, headache, dizziness, nausea, vomiting, mental fatigue and bluish tinge on the skin and mucous membranes.
- Anaemic hypoxia : It results from the reduced oxygen-carrying capacity of the blood due to anaemia (decreased haemoglobin content in blood) or carbon monoxide poisoning (some haemoglobin occupied by CO). In both cases, less haemoglobin is available for carrying oxygen.
- Asphyxia (Suffocation) : The O2 content of blood falls and the CO2 content rises and paralyses the respiratory centre. Breathing stops and death occurs.
- Common cold : Disease-causing microbes present in the air attack respiratory tract, producing inflammation of the mucous membrane. Rhinitis is a chronic or acute inflammation of the mucous membrane of nose.
- Rhinitis in the nasal chambers.
- Sinusitis in the sinuses.
- Pharyngitis in the pharynx, often called sore throat, and is usually accompanied by tonsilitis (enlargement of tonsils).
- Laryngitis in the larynx, causing a hoarse voice and difficulty in speaking.
- Bronchitis in the bronchioles.
- Bronchitis : It is caused by the permanent swelling in the bronchi. As a result of bronchitis, cough is caused and thick mucus with pus cells is spitted out. The patient experiences difficulty in breathing.
- Pneumonia : During pneumonia, oxygen has difficulty in diffusing through the inflamed alveoli and the blood pO2 may be drastically reduced. Blood pCO2 usually remains normal because CO2 diffuses through the alveoli more easily than O2. This disease is caused by Streptococcus pneumoniae, other bacteria, fungi, protozoans, viruses and the patient feels difficulty in breathing. Its prominent symptoms are trembling, pain in the chest, fever, cough etc. This disease is prevalent in either children or elderly persons in old age.
- Lung cancer : It is believed that due to excess smoking, lung cancer (carcinoma of lungs) is caused. The tissue increases limitlessly, which is called malignancy. This disease is fatal. The frequency of occurrence of this disease in smokers is 20% more. Malignancy of tissues (neoplasia) causes pressure on the cells of other tissues and destroys them. The blood capillaries are ruptured, blood starts flowing and death is caused by excessive bleeding.
- Tuberculosis (TB) : It is caused by bacteria Mycobacterium tuberculosis. These bacteria settle in lungs at different places and convert normal tissue into fibrous tissue. Since the respiratory surface is decreased, the difficulty in breathing is also experienced. If the patients start taking medical advice and the medicines right from the initial stage regularly, the patients can be fully cured of the disease.
Now a days, a new therapy DOT (Direct observed treatment) is used for tuberculosis treatment, recently launched by Indian Government. Many other drugs like rifampin and isoniazid are successful for the treatment of tuberculosis. Tuberculosis bacteria spreads by inhalation and exhalation.
NOTES
- In elephant, false vocal cords are absent.
- In hippopotamus, true vocal cords are absent.
- In birds, sound is produced by syrinx.
- Sound of rabbit is called as quacking.
- In normal respiration.
Frog show - 35% cutaneous respiration
- 9% Buccopharyrngeal respiration
- 56% Pulmonary respiration.
- Drinker's Respiration or Tank Respiration is an iron lung invented by Philip Drinker, an American Engineer, in 1929.
- A dark bluish colour of skin and mucous membrane due to deficiency of oxygen in the blood is called cyanosis.
- In frog, sternohyal and petrohyal muscles are related with the process of respiration.
- Lodwing first explained gaseous exchange in blood.
- Rima glottides is the gap between the vocal cords.
- The vocal cords are made up of yellow elastic tissue covered by non keratinized stratified squamous epithelium.
Post a Comment